Spotlight on Naloxone Co-Prescribing
This is a guest post by Adm. Brett Giroir, Jessica White, Teresa Manocchio, Sean Klein, Zeid El-Kilani. Adm. Brett Giroir is the 16th Assistant Secretary

This is a guest post by Adm. Brett Giroir, Jessica White, Teresa Manocchio, Sean Klein, Zeid El-Kilani. Adm. Brett Giroir is the 16th Assistant Secretary
There’s been a lot of discussion about differences in susceptibility and symptom severity among people with different blood types. Does your blood type determine how
The following originally appeared on The Upshot (copyright 2020, The New York Times Company). American opponents of proposed government-run health systems have long used the
Paul Shafer is an assistant professor of health law, policy, and management at the Boston University School of Public Health. Nicole Huberfeld is a professor
This is part 4 in our series on the opioid crisis, presented with support from the NIHCM Foundation. We’ve talked about the state of the
Part 3 of our opioid series, supported by the NIHCM Foundation, examines the potential of marijuana to improve outcomes in opioid addiction therapy. Some studies
There is an unsatisfactory complacency that emerges from believing not being racist is adequate. It’s not adequate. In truth, it’s a passivity that tacitly supports structural racism everywhere, including in HSR. That I was not racist was merely a story I told myself. It didn’t have any impact on my community or the institutions where I work.
In recent years, life expectancy in the US has dropped, and deaths of despair have been a significant contributor. Drug overdoses and suicides have increased
Moving the needle on upcoding will require a multifaceted approach, dependent on both regulatory oversight and buy-in from payers and providers.
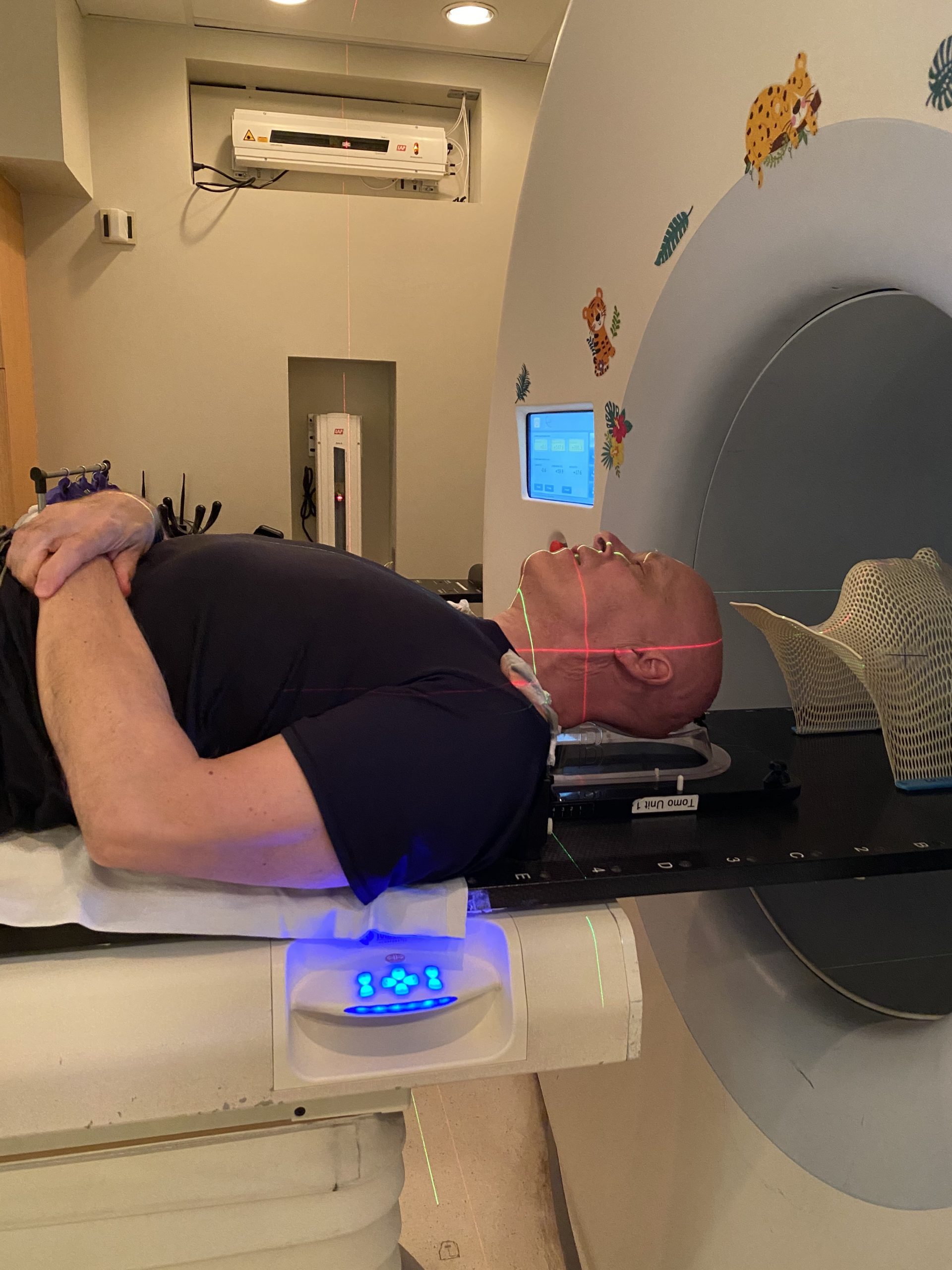
In a previous post, I walked you through my decision to have radiation therapy only, without chemotherapy. Now I’ve started therapy. This post is about
Specifically, providers and payers can sometimes hide behind that complexity to intentionally bill erroneously. Upcoding is one potentially fraudulent form of billing. Upcoding occurs when more intensive and expensive diagnoses or treatments are documented than what was actually provided to the patient or medically necessary.
In 2016, Healthcare Triage presented a special series of videos examining the opioid crises in the United States. Now, we’re taking another look at the