
Nambi J Ndugga (@joerianatalie) is a policy analyst with the Boston University School of Public Health. Research for her piece, below, was supported by the Laura and John Arnold Foundation.
The Centers for Medicare & Medicaid Services (CMS) has proposed the International Pricing Index (IPI) model as a way of addressing the rising costs of prescription drugs for Medicare beneficiaries. What is it and how would it work? First some background:
How is Medicare’s drug coverage currently structured?
Medicare offers prescription drug coverage to its beneficiaries in two of its four parts: Part B (provider-administered drugs) and Part D (self-administered drugs). Though IPI would apply only to the former, it’s worth putting it in the context of all of Medicare drug coverage and spending, including Part D.
The optional Part D covers self-administered prescription drugs. It does not include over the counter (OTC) drugs or weight loss/gain treatments. Part D drugs are paid for by private insurance plans that negotiate prices with drug manufacturers (or contract with pharmacy benefit management organizations to do so on their behalf). Medicare is prohibited from interfering with any price negotiations.
Since Part D’s implementation in 2006, there has been a tenfold increase in Medicare’s pharmaceutical spending, which is due to the rise of high cost specialty drugs in the market. (Specialty drugs are those with a negotiated price of $670 or more per month.) It is estimated that two thirds of all Part D spending will soon be due to these drugs.
Medicare Part B is also optional. It covers, among other things, prescription drugs administered in hospital settings and those delivered via durable medical equipment, such as nebulizer treatments. Part B also covers certain outpatient drugs such as flu and pneumococcal vaccinations. For the few outpatient drugs covered by Part B, Medicare requires the beneficiary pay 20% of the approved price.
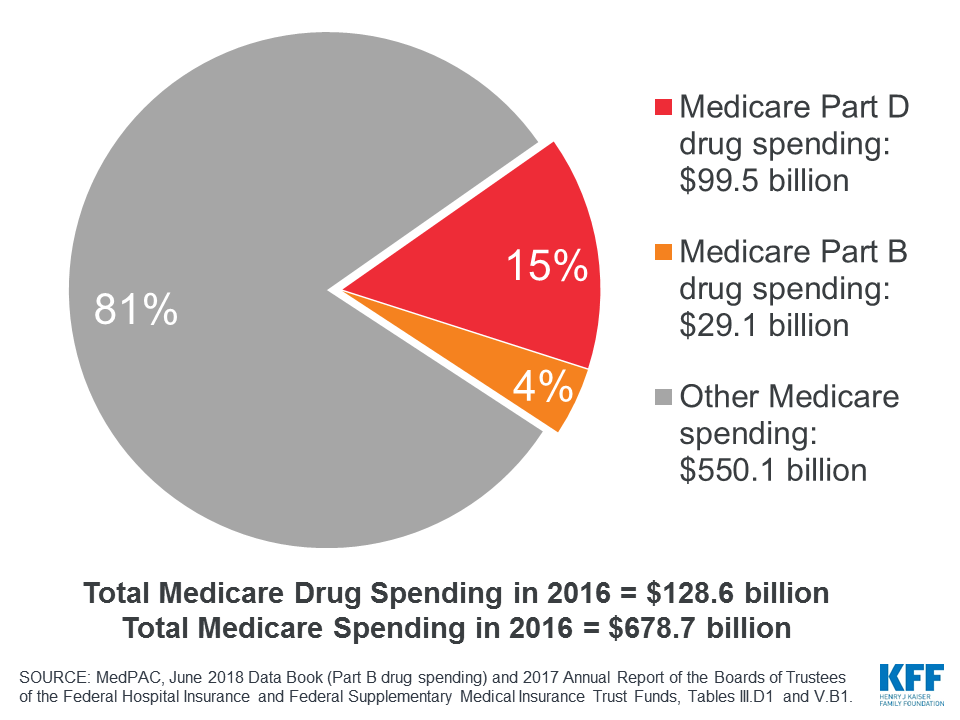
Part B drugs are individually more expensive, but Medicare spends more on Part D simply because Part D covers more. In 2016, Medicare Part D spending accounted for 15% of all Medicare spending and Part B accounted for 4%.
{kind=link}
What is the IPI model?
The IPI model was proposed by CMS to address Medicare’s high pharmaceutical spending, targeting single source drugs and biologics which account for 84% of Part B drug spending.
There are two parts to the IPI model. This post will focus on the first part, which sets target sales prices for select physician-administered drugs. The model aligns Medicare’s pricing with that of 16 comparable foreign countries: Austria, Belgium, Canada, Czech Republic, Finland, France, Germany, Greece, Ireland, Italy, Japan, Portugal, Slovakia, Spain, Sweden, and the United Kingdom.
Why focus on Medicare Part B?
Even though Medicare spends more on Part D, Part B per beneficiary expenditures have grown at a much faster rate. From 2006 to 2011, Part B per beneficiary expenditures grew by 7.1% while Part D per beneficiary expenditures grew by 3%. In the following five-year period (2012-2017), Part B and Part D per beneficiary expenditures grew by 11.1% and 3.2%, respectively.
The ten most expensive Part B drugs are all biologics — medicines made from living organisms, including gene and cell therapies, monoclonal antibodies, and vaccines — that treat diseases such as cancer, arthritis, and ocular degeneration. Most biologics are single source drugs — effectively, market monopolies — which makes it difficult to reduce prices through negotiation.
Spending on Part B drugs doubled between 2009 and 2017, with spending on specialty drugs increasing by 1000% over the past decade. The Department of Health and Human Services (HHS) found that the drug manufacturers, wholesalers, and distributors charge the United States 1.8 times higher prices for these Part B drugs than they do other countries. HHS concluded that Medicare could achieve significant savings if Part B drug prices in the US were similar to those in other comparable countries.
How does Medicare currently set Part B drug prices?
Under current law, HHS is prohibited from negotiating directly with pharmaceuticals on behalf of Medicare. Medicare reimbursements for most Part B drugs are based on the drug’s average sales price (ASP) and an additional six percent markup, reduced to 4.3% markup for most drugs in 2013 due to the Budget Control Act of 2011. However, for single-source drugs, the price is still set at ASP plus a six percent markup. When the ASP is not available for the drug (often the case for new drugs), CMS uses the wholesale acquisition cost (WAC) instead.
How could the IPI model impact Medicare spending?
Preliminary estimates from HHS suggest that the IPI model could reduce Part B expenditures by 30% for single source drugs and biologics. However, analysis by Avalere Health found that less than one percent of Medicare enrollees would see a reduction in out-of-pocket costs. Concerns raised about the model include that it could reduce drug innovation, that it is unclear what would happen if a drug company refuses to provide a drug at the IPI price, and that the hospitals in another drug discount program (340B) would end up spending more, not less, for drugs.
The IPI model would be phased in over five years (2020-2025), and focus on physician practices and hospital outpatient departments in select geographic locations (TBD), reflective of a representative 50% of Medicare Part B expenditures. This will allow Medicare to monitor and evaluate the model during this period and determine whether international pricing standards can reduce spending while maintaining beneficiary access and quality of care.
Conclusion
While there is considerable interest in reducing Medicare’s prescription drug spending, no proposals have been enacted. When the IPI model is implemented, we will be able to observe the impacts it has on Medicare expenditures and the prices of Part B single-source and biologic drugs.