
Eline van den Broek-Altenburg, PhD, has served as a health policy advisor in the Dutch and European parliaments and is currently an assistant professor at the Larner College of Medicine at the University of Vermont. Follow her on Twitter at @E_line and #ReDoTheMath.
Adam Atherly, PhD, is a professor and director of the Center for Health Services Research at the Larner College of Medicine at the University of Vermont. Twitter: @AdamAtherly
While a growing number of people are starting to understand the message of the intuitive picture of “Flattenin g The Curve”, some health economists are starting to wonder how flat the curve should actually be for the benefits to exceed the costs. Since the graph went viral on social media on February 28, media and citizens alike are calling for a slowing down of the spread of COVID-19. (The curve was first published in a 2007 paper by the Centers for Disease Control and Prevention [CDC].)
g The Curve”, some health economists are starting to wonder how flat the curve should actually be for the benefits to exceed the costs. Since the graph went viral on social media on February 28, media and citizens alike are calling for a slowing down of the spread of COVID-19. (The curve was first published in a 2007 paper by the Centers for Disease Control and Prevention [CDC].)
But how does the economic cost of the flattening fit into the discussion? The New York Times reported that the “self-quarantine” decision by both the U.S. and the U.K. government was hugely influenced by an epidemiological study from Imperial College. That study didn’t consider the cost of the different policy options — just the health impacts. The value of policies with health impacts are typically compared to their cost using a standard “cost effectiveness” framework. Below, we use publicly available data to calculate the cost effectiveness of the flattening the curve.
The Cost Effectiveness of the Self-Quarantine
When considering the value of a healthcare intervention to inform decision-making, benefits are usually measured in terms of life years gained, with the life years adjusted for the “quality” of the life (using standard formulas) to create a “Quality Adjusted Life Year” or QALY. For an intervention, the QALYs gained are added up and adjusted for differences in when the gains occur.
One of the key numbers in these models is the number of years of life a typical person will be expected to survive. This is why interventions in younger populations will typically yield more QALYs than interventions in older populations: because younger people have longer life expectancy. The formula for QALY calculation is:
Years of Life x Utility Value = #QALYs
where Utility Value is a number between 0 and 1 that captures the average quality of life during those years (1 for perfect health and lower for worse states of health).
Heath systems then compare the QALYs gained to the cost and calculate a cost per QALY gained. In the United States, interventions that cost less than $100,000 per QALY gained are often considered “cost effective,” although the precise number is somewhat controversial. The National Health Service in the U.K. often uses 30,000 pounds per QALY as a benchmark, although there is nuance in the precise threshold.
So, is the current “stay at home” and social isolation-policy, with school closed and businesses shuttered, cost effective using the standard health economics framework?
Calculate the Gains
The years of life-gains are relatively straightforward. Even if we are suspicious of death rates and incidence rates currently being reported (because we do not know how accurate the denominators of those ratios are), statistics on the people who died of COVID19 in China and Italy are the best source of currently available data. The Italian National Health Institute pegged the median age of death from COVID-19 in Italy at 80.5. This is consistent with early data from the United States.
(Note that studies of this type typically use means rather than medians. We did not find any data we felt was reliable with mean age of death. However, the reported age distributions suggest that the mean and median should be reasonable close).
The average 80-year old in the United States has a life expectancy of about 9 years, suggesting that on average, a death averted will “buy” 9 extra years of life. In QALY-estimations, this number needs to be adjusted for the “quality of the years”. In Italy, 99% of deaths had an underlying pathology that needs to be incorporated in QALY adjustments. If we use diabetes as a reasonable proxy for the many chronic diseases, we would adjust the 9 years down to 7.8 years or QALYs. In other words: the average loss per person of quality-adjusted life years is 7.8.
The last ingredient we need to calculate the QALY-gains is also the most controversial of data reporting of the past few weeks: the number of deaths. When we multiply 7.8 with the number of people who will die, we get the QALY loss. According to a CDC scenario analysis, the expected range of deaths is from 200,000 to 1.7 million people. This implies the pandemic, if unchecked, will lead to a loss of between 1.56 million and 13.26 million QALYs.
Calculate the Costs
What, then, is the cost of the intervention of social distancing? One easy estimate would be to use the cost of the current stimulus bill before congress — 1 trillion dollars. This is likely an underestimate of the true cost, but is a reasonable starting place. If the stimulus becomes 4 trillion dollars, the cost per QALY gained will be significantly higher. In the figure below we show the ranges we calculated for the two scenarios.
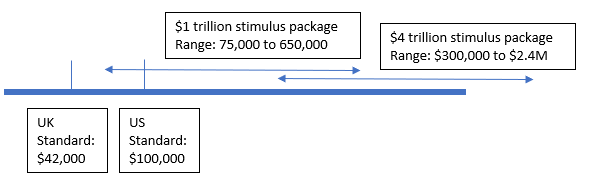
We calculated the cost per QALY gained from the current approach to be somewhere between approximately $75,000 and $650,000. We did this by dividing the planned stimulus package by the QALYs gain we estimated. This is somewhere between reasonably cost effective and clearly not a wise investment if we used the conventional standard cut-off point of $100,000 per life year gained. If the total investment was $4 trillion, the cost per QALY gained would rise to a range of $300,000 to $2.5 million per QALY gained — an expenditure far out of line from other healthcare investments.
Why haven’t these numbers been publicly calculated and debated?
Now, this “health economics 101” version of doing the math is of course far from perfect which is largely due to the uncertainty around the data inputs. In particular, the key variable is the expected number of deaths. A pandemic that is likely to lead to 1.7 million deaths can justify the enormous public costs. However, if the pandemic is in the lower end of the predicted range, then the public funds would have been more valuable if spent elsewhere. One important element of this is the uncertainty (risk) about how infections and deadly COVID-19 will ultimately be, which might make it rational to be more cautious than one might be ordinarily. This emphasizes that one priority should be the rapid collection of additional data and updates to prediction models.
Some claim it is impossible or even unethical in times of a crisis, to think about cost when lives are involved. But in a world of finite resources, it’s necessary to make choices. Why not use a framework that has been defended by governments and scientists for decades to justify treatment and health reimbursement systems’ decisions to not pay for life saving treatments? The entire point of the exercise is to help make hard choices systematically based on data.
In theory, if decision rules like cost effectiveness represent sensible approaches to making policy choices, health economists should be out front helping guide policy. Our calculations suggest that current strategies will be cost effective only if the predicted mortality rates are at the top of the predicted range and costs are at the bottom of the range – a combination of worst care / best case that is unlikely. Consideration of targeted mitigation strategies that minimize the economic cost while protecting the most vulnerable are warranted.
UPDATE: A number of readers have commented on our use of the economic stimulus package as the “cost” of the shutdown. As readers have correctly noted, much of the stimulus is a transfer, which ordinarily wouldn’t be considered a cost. However, this may be a unique situation. The stimulus is intended — at least in part — to replace income for companies forced to shut down. That lost income is the correct measure — it’s the forgone productive activity that didn’t happen due to the shutdown. If the government accurately estimated the reduced productivity by firms and transferred that amount of money, that would the right number. Other costs in the stimulus that are intended to directly fight the pandemic would not necessarily belong in the cost calculation because those are costs that presumably would happen with or without the shutdown.
So is $1T the right number? A recent Wall Street Journal editorial suggested a 25% reduction in GDP due to the shutdown — which would be about $875B per month. A recent Fed report suggested a similar number. It is likely that our $1T is quite low and an estimate of more like $2T may be called for, in line with the now $2.2T relief package. The biggest cost may actually be small business failures that are permanent. We have an estimate of that number, and it is on the order of triple the cost of the stimulus.
We tried to be very conservative in our estimates throughout and essentially found that the shutdown is only justified using conventional CEA benchmarks in a very limited combination of the worst predicted health outcomes and the lowest costs. The cost parameters may be variable, but other inputs are not going to drastically change that conclusion.
A number of other readers have suggested that there will be negative health outcomes associated with the shutdown and unemployment. There is a body of literature supporting that argument, but when we ran the calculations, even a relatively high value for the health impact of unemployment — decreasing QALYs by 10% — coupled with a very high unemployment rate — we used 20% — is an order of magnitude lower than the life years lost due to deaths unless unrealistic assumptions are made about unemployment duration.