
Allison R. Kolbe, Ph.D. is an Oak Ridge Institute for Science and Engineering Fellow at the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Sean A. Klein, Ph.D. is a Presidential Management Fellow at the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation.
The COVID-19 pandemic has resulted in over 6 million infections and more than 200,000 deaths in the U.S. alone, and has exposed long-standing health disparities through its disproportionate impact on racial and ethnic minority communities. These disparities are likely due to a complex combination of risk factors, such as the presence of comorbidities, discrimination, healthcare access and utilization, occupation, or other social determinants of health. As the pandemic continues, understanding the presence and extent of this disproportionate impact remains an area of active and ongoing research. Here, we provide a current snapshot of COVID-19 case and mortality demographic data at state and, where available, tribal and county levels with a focus on identifying and quantifying racial disparities. A more detailed report is available here.
Data availability and limitations of demographic data for COVID-19 outcomes
An important first step to understanding whether and where disparities in COVID-19 outcomes exist is understanding the available data. Data reporting on the racial/ethnic demographics of COVID-19 cases and deaths has improved significantly since the early months of the pandemic (Exhibit 1).
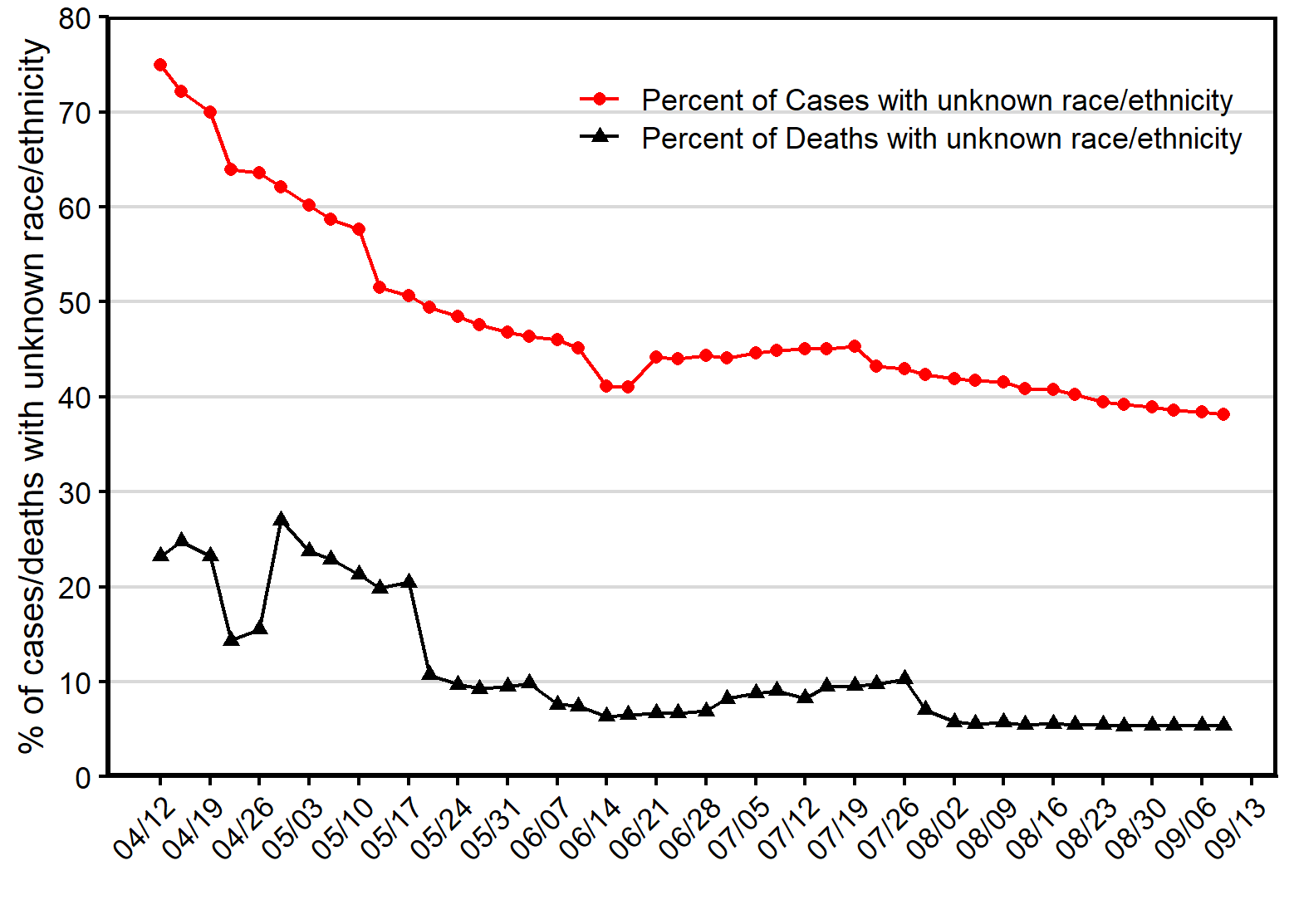 As of September 9, 2020, all 50 states and the District of Columbia were reporting data on COVID-19 infections and/or deaths by race and/or ethnicity. While the number of states reporting race and ethnicity demographics for COVID-19 cases and deaths has improved significantly since April, about 38% of all COVID-19 cases and 5% of COVID-19 deaths lack associated race or ethnicity data. Far fewer states report race and ethnicity for other relevant metrics: only 7 states reported race and ethnicity for testing, and 17 for hospitalizations.
As of September 9, 2020, all 50 states and the District of Columbia were reporting data on COVID-19 infections and/or deaths by race and/or ethnicity. While the number of states reporting race and ethnicity demographics for COVID-19 cases and deaths has improved significantly since April, about 38% of all COVID-19 cases and 5% of COVID-19 deaths lack associated race or ethnicity data. Far fewer states report race and ethnicity for other relevant metrics: only 7 states reported race and ethnicity for testing, and 17 for hospitalizations.
In addition to many COVID-19 metrics lacking associated race and ethnicity data, data are particularly limited for Asian, Alaska Native/American Indian (AIAN), and Native Hawaiian/Pacific Islander (NHPI) populations. Many states do not report data for these groups, and data reporting for AIAN populations is further complicated by overlapping state, tribal, and county reporting jurisdictions. These data limitations represent a considerable challenge to measuring disparities in COVID-19 outcomes among minorities.
Racial and ethnic disparities in COVID-19 cases and deaths
As more data have become available, the disproportionate impact of COVID-19 on minority communities has become clear. Using data from the COVID Tracking Project, we quantified disparities in COVID-19 cases and deaths. We used this data to explore the disparity landscape across the U.S. among the U.S. Census Bureau’s racial and ethnic categories (Black, Asian, Alaska Native/American Indian, Native Hawaiian/Pacific Islander, White, and Latino/Hispanic).
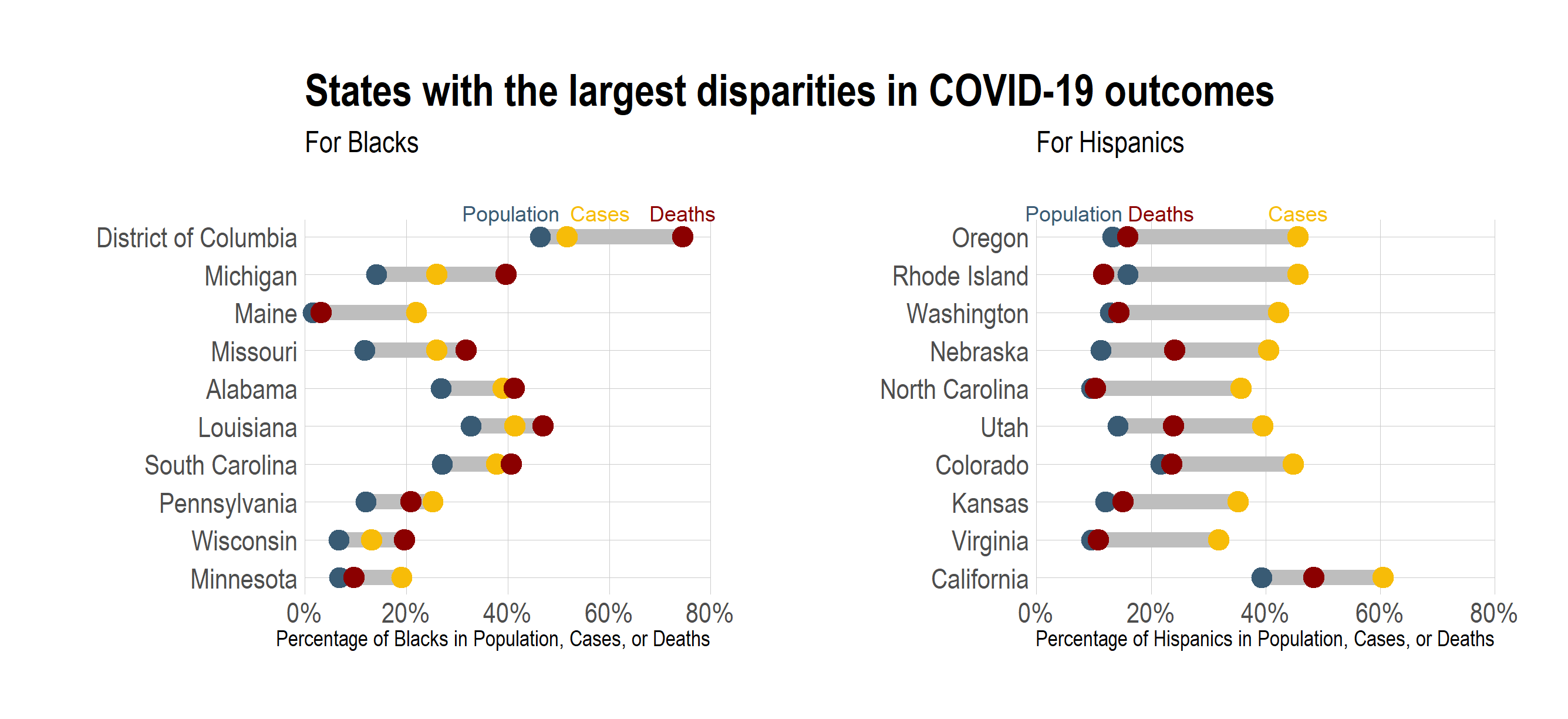
Large disparities exist in COVID-19 outcomes among the two largest racial/ethnic groups, Blacks and Hispanics. Exhibit 2 shows the states with the largest absolute difference between the population of Blacks or Hispanics and their proportion of either cases or deaths. For Blacks, several of the states with the largest disparities for COVID-19 cases have even larger disparities for COVID-19 deaths. In contrast, Hispanics are significantly overrepresented in COVID-19 cases in many states, but disparities in COVID-19 deaths for Hispanics tend to be smaller.
However, this does not mean that Hispanics do not experience severe illness due to the coronavirus — in fact, Hispanics are overrepresented in nearly all of the 16 states currently reporting ethnicity for hospitalizations. Despite disparities in COVID-19 outcomes, Blacks make up a near-proportional number of tests in 7 reporting states, and Hispanics in 6 out of 7 reporting states. Given that Blacks and Hispanics make up a greater than proportional number of COVID-19 cases, this likely means that Blacks and Hispanics are being under-tested.
Data on COVID-19 outcomes are more limited for Asians, Alaska Native/American Indian, and Native Hawaiian/Pacific Islander (NHPI) populations. However, where data are available, we found that disparities exist for these populations as well. For Asians, disparities in both COVID-19 cases and deaths are present in some states, but are not as geographically widespread as the disparities observed for Black and Hispanic populations. In Hawaii, NHPI make up approximately 10% of the population but 43% of COVID-19 cases. Similarly, a disproportionate impact of COVID-19 has been observed in AIAN populations. As an example, the Navajo Nation has experienced a particularly high case burden, with over 5% of the population contracting COVID-19 by July, compared to 2.7% of New York City residents at that time. Furthermore, disparities in AIAN populations can be seen throughout AIAN populations in Arizona.
In contrast to the widespread disparities observed for minority populations, non-Hispanic Whites are underrepresented in COVID-19 cases and deaths in the majority of U.S. states, and also experience lower hospitalization rates than minority populations.
State-level data doesn’t tell the whole story
More granular data can provide greater insight into the presence and extent of racial and ethnic disparities in COVID-19 outcomes. We collected race and ethnicity demographics for COVID-19 cases from the Department of Health websites of six states: Arizona, Florida, Illinois, Louisiana, Mississippi, and Virginia. In all cases, we observed considerable variation in the size of disparities between counties. Furthermore, in all six states, larger proportions of one or more minority groups were associated with higher COVID-19 case burden (defined as the percentage of the county population that has tested positive). However, case burden was not associated with population size, indicating that these results cannot be explained by minority prevalence in urban counties. These results are consistent with other recent studies that have shown a disproportionate number of cases occur in areas with large minority populations.
Ongoing challenges and conclusions
Currently available data indicate significant, widespread disparities in COVID-19 cases and deaths for Black, Hispanic, and American Indian populations, and suggest that disparities may also exist in some locations for Asian and Native Hawaiian/Pacific Islander populations. However, many data gaps and challenges remain for evaluating the nature of these disparities. Although data reporting on race and ethnicity has improved considerably, nearly 38% of all COVID-19 cases as of September 2020 did not have associated race and ethnicity data.
Inconsistency in the race/ethnicity categories used also hinders comparisons to existing population data. Although state-level data are insufficient to fully characterize the impact of COVID-19 on minority communities, data are extremely limited at county or municipal levels. With county-level data from six states, we observed that disparities persist in rural, suburban, and urban counties and counties with high minority population tend to have high COVID-19 case burden. Efforts to improve data reporting, comprehensiveness, and granularity will be critical to understand the impact of COVID-19 on minority populations. Linking this information to social determinants of health data will provide further insight into the causes and potential policy solutions to address racial and ethnic disparities in the COVID-19 pandemic.