
In the last 20 years, many employers shifted a larger percentage of health care costs to employees and called it cost control. Increasing the beneficiary’s cost sharing is relatively easy to do, and it controlled the employer’s costs, but not the overall costs. By tying USG health expenditures to a percentage of GDP, Ryan’s proposal essentially block grants Medicaid and caps Medicare government expenses to a voucher level. Who does the hard work of cost control? The IPAB would be repealed. We’re left with private plan competition. What’s been the record on that tool the last few decades? From the CBO Analysis of the Ryan proposal (at 23):
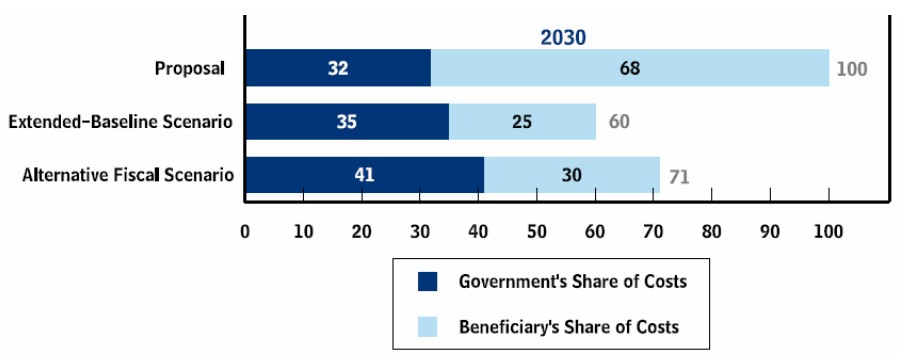
To summarize, a typical beneficiary would spend more for health care under the proposal than under CBO’s long-term scenarios for several reasons. First, private plans would cost more than traditional Medicare because of the net effect of differences in payment rates for providers, administrative costs, and utilization of health care services, as described above. Second, the government’s contribution would grow more slowly than health care costs, leaving more for beneficiaries to pay.
How much more for a 65 year old? A lot: CBO projects that total Medicare health expenditures will rise significantly under Ryan’s proposal; the Extended-Baseline Scenario shows total health expenditures that are 40% lower. Translated: Ryan’s proposal doesn’t address long-term cost control, it just shifts those costs to beneficiaries.
Justin Anderson had similar thoughts in this comment.
