
Atul Gawande introduced us to McAllen, TX:
The streets are lined with palm trees and pickup trucks. McAllen is in Hidalgo County, which has the lowest household income in the country… McAllen has another distinction, too: it is one of the most expensive health-care markets in the country.
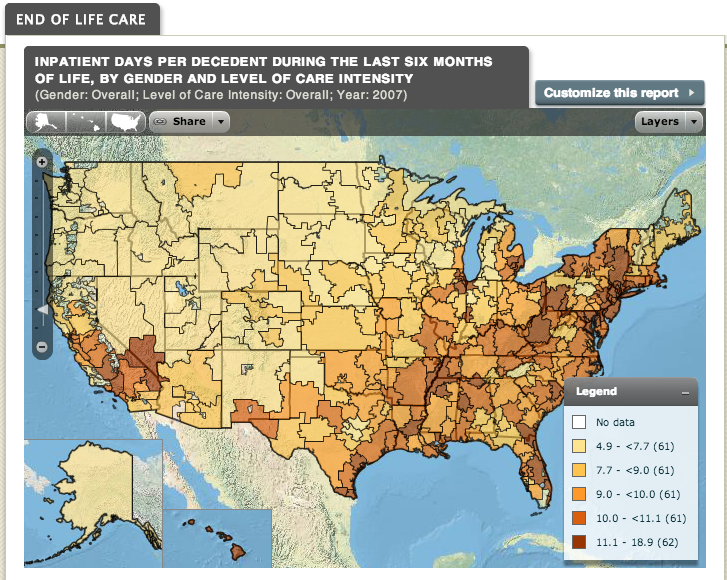
Gawande called attention to the striking variation across America in the volume and intensity of medical services delivered to patients with similar health status. For example, here is a map of variation in how many days patients spend in the hospital at the end of their lives, from the Dartmouth Atlas.
Evidence shows, however, that sometimes more intensive treatment does not produce better patient outcomes. One strategy for reducing the cost of US health care is to standardize medical practice around practices that achieve the best outcomes without unnecessary interventions.
To get there, however, we need to understand why treatment intensity varies across the country. For example, it might be that in Florida people spend more days in the hospital at the end of their lives compared to people in Oregon, because Floridians want that more than Oregonians do.
Amitabh Chandra drew my attention to a cool study by David Cutler, Jonathan Skinner, Ariel Dora Stern, and David Wennberg that looks at the relationship between regional variation in health care spending, on the one hand, and physician and patient preferences for intensity of treatment, on the other.
Cutler and his colleagues measured regional variation in patient preferences for more intensive treatment using a survey of Medicare enrollees asking about whether they would want aggressive care interventions. They measured physician preferences through another survey that presented doctors with vignettes asking how they would treat patients. For example, a vignette that
asks how frequently the physician would schedule routine follow-up visits for patients with stable angina whose symptoms and cardiac risk factors are now well controlled on current medical therapy.
There are no guidelines that indicate that follow-up of stable angina should be more often than every four months, yet 23% of cardiologists recommend this. In general, physicians erred on the side of recommending more treatment than evidence-based guidelines support.
Moreover, regional variation in spending is strongly associated with regional variation in physician preferences for more intensive treatments, but not with patient preferences.
We find patient demand is relatively unimportant in explaining variations. Physician organizational factors (such as peer effects) matter, but the single most important factor is physician beliefs about treatment: 36 percent of end-of-life spending, and 17 percent of U.S. health care spending, are associated with physician beliefs unsupported by clinical evidence.
This finding was predicted by Kenneth Arrow, who was the first to point out that in medicine, the consumer is highly uncertain about the relative values of alternative courses of treatment. Lacking information, she is likely to rely on the preferences of her physician. Physicians, however, believe in their treatments and make money by supplying them, and thus have an incentive to overtreat.
Every school of health policy has a point of view about how to address this problem. I will just point out that this finding underlines the importance of the socialization of physicians’ attitudes about responsible treatment and use of medical resources. In particular, we need to address the issues raised by the American College of Physicians, in their revised ethical manual:
Physicians have a responsibility to practice effective and efficient health care and to use health care resources responsibly. Parsimonious care that utilizes the most efficient means to effectively diagnose a condition and treat a patient respects the need to use resources wisely and to help ensure that resources are equitably available.
This ethic has been discussed several times on TIE (here, here, here, and here) and on my previous blog here.
